Importance: Improved treatments for combat-related posttraumatic stress disorder (PTSD) are needed.
Objective: To determine whether navigated transcranial magnetic stimulation (TMS) is efficacious when added to intensive residential therapy for combat-related PTSD.
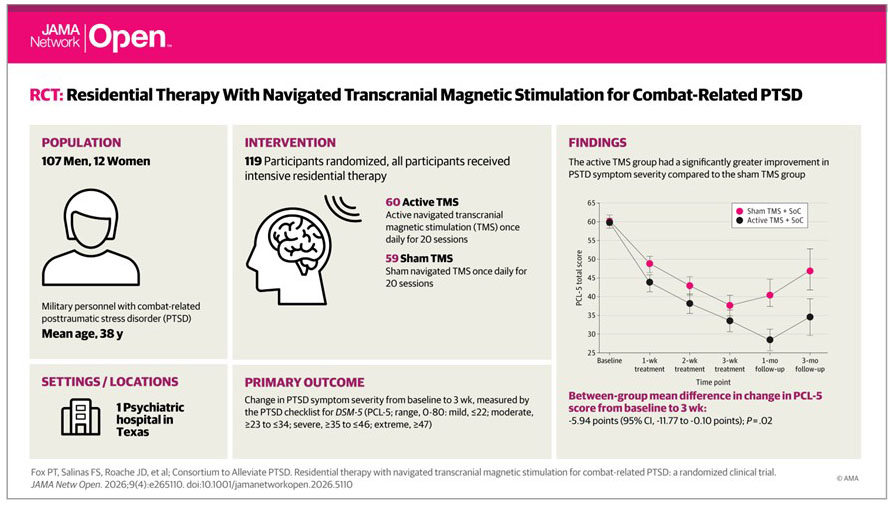
Design, Setting, and Participants: A 1:1 randomized clinical trial with 30-day treatment and 1- and 3-month follow-ups was conducted in a residential facility specializing in military mental health with geographically broad catchment. Enrollment was from July 2017 to March 2019. Participants were military personnel with PTSD recruited from treatment facility admissions. Patients, staff, and assessors were blinded to treatment arm. Data were analyzed from November 2020 to April 2023.
Interventions: Both trial arms received intensive residential treatment as standard of care (SoC). SoC included manualized prolonged exposure twice per week combined with daily, day-long psychotherapeutic augmentations as a 30-day program. Navigated TMS (active or sham) was added to SoC. TMS was individually targeted both anatomically (structural) and connectomically (functional) using magnetic resonance imaging and delivered by robotic stereotaxy. TMS was delivered daily (7 d/wk) for up to 20 sessions.
Main Outcomes and Measures: The primary outcome was symptom-severity change in PTSD Checklist for DSM-5 (PCL-5) scores between baseline and end-of-treatment assessments. Secondary outcomes were Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) and Patient Health Questionnaire–9 (PHQ-9) depression module scores across treatment and follow-up phases.
Results: Among 129 military personnel and veterans screened, 119 with moderate (9 [8%]), severe (56 [47%]), or extreme (54 [45%]) PTSD were randomized (60 to active TMS and 59 to sham TMS), with 6 dropouts (5%) before end of treatment. Mean (SD) participant age was 37.6 (6.5) years; 107 (90%) were male. For both treatment arms, all measures confirmed significant symptom relief relative to baseline. At end of treatment, both PTSD measures showed superior symptom relief for active TMS: mean PCL-5 score difference, −5.94 (95% CI, −11.77 to −0.10; P = .02); mean CAPS-5 score difference, −6.03 (95% CI, −10.84 to −1.22; P = .008). In follow-up, 2 measures showed superior symptom relief durability for active TMS: PCL-5 (mean score difference, −12.30; 95% CI, −22.03 to −2.57; P = .008) and PHQ-9 (mean score difference, −3.45; 95% CI, −0.03 to −6.86; P = .03). Reliable change indices showed superior symptom relief durability for active vs sham TMS on the PCL-5 (85% [95% CI, 71%-98%] vs 59% [95% CI, 41%-78%] at 1 month; P = .03).
Conclusions and Relevance: In this randomized clinical trial of combat-related PTSD, navigated TMS was efficacious when added to intensive residential treatment. This suggests that navigated TMS neuromodulation can effectively reduce PTSD symptoms.